 |
||||
|
Rocky: The Gecko That Loved to Eat Sand Case report by Dr. Craig Stanton
On presentation Rocky was bright alert and responsive and readily bit Dr. Craig while he performed a physical exam. Her temperature was measured via infrared thermometer to be 83F and her respirations were 12 breaths per minute. She had a thin tail, distended hard abdomen and slightly pale mucous membranes but her physical exam was otherwise within normal limits. She weighed 29g. Our initial assessment was that Rocky had a sand impaction and our suspicions were confirmed by a ventral dorsal radiograph. A large amount of mineral density material filled the caudal abdomen in three to five large clumps. Given the degree of impaction and her otherwise healthy condition, we recommended immediate surgery. Understanding the risks of surgery, the owner elected to try medical management for some time to see if he could get a bowel movement. We recommended 90F water soaking and gentle massage and tube feeding a small amount of lactulose with the goal of an eventual enema if nothing changed. Overnight the gecko seemed no different and perhaps was getting weaker. The owner was briefed about the poor prognosis for medical management and our lack of experience with gecko ceiliotomy/enterotomy surgery and we all decided to take Rocky to surgery.
An isoflourane induction was achieved in a small chamber and then maintained with a syringe case mask packed with cotton. Ventilations were performed 4 breaths per minute and the operating platform consisted of two 100F saline bags covered with a surgical towel in order to maintain body temperature of 90F. Rocky's belly was prepped with a nolvasan scrub and betadine.
The ceolomic peritoneum was closed with 6-0 vicryl and the skin was closed with 7-0 ethilon using an everting horizontal mattress pattern. Five cruciates were also placed above the horizontal mattress to keep the everted skin apposed well.
Rocky's owner took her home and kept her moist with warm paper towels as a substrate. She was NPO overnight but offered two small crickets the following afternoon. She ate these with a voracious appetite and the number of crickets offered each day increased until she was eating 6 crickets per day. Rocky's six week recheck revealed that the skin sutures had been shed and the incision was looking good. Her tail base had grown and she was looking very much improved. Rocky continues to be housed on paper towels as substrate and continues to have a voracious appetite. Rocky continues to do well at the time of this article, six months post operative, and her tail base continues to grow. As far as we know, Rocky is the only gecko to survive a a sand impaction surgery.
Possible
good things: Very good sedation from the pre-anesthetic medications,
good mu-agonist provides the best pain control. Patient was still very
full of life prior to and up until surgery, not down and out yet. |
||||
 Rocky
is a young leopard gecko and presented with a history of decreased appetite
for the last month, shrinking tail and anorexia. Her owner had her for
four months prior to onset of clinical signs. Initially, Rocky was a
great eater but for the last month she had not been eating much at all.
Also, in the last week, she had no bowel movements. The husbandry seemed
adequate and two other geckos in the collection were doing fine. The
temperature gradient was about 95 to 75 with an under the tank heater
on one side. Rocky's owners had been gut loading meal worms and crickets
right before feeding and there is an infrared night light. Rocky's cage
substrate was a fine calcium sand marketed as safe for this species.
Rocky
is a young leopard gecko and presented with a history of decreased appetite
for the last month, shrinking tail and anorexia. Her owner had her for
four months prior to onset of clinical signs. Initially, Rocky was a
great eater but for the last month she had not been eating much at all.
Also, in the last week, she had no bowel movements. The husbandry seemed
adequate and two other geckos in the collection were doing fine. The
temperature gradient was about 95 to 75 with an under the tank heater
on one side. Rocky's owners had been gut loading meal worms and crickets
right before feeding and there is an infrared night light. Rocky's cage
substrate was a fine calcium sand marketed as safe for this species.
 Preoperative
care consisted of a 90F water soaking and dry-needling acupuncture,
approximating bilateral points BL21 and BL25. Needles used were 0.18mm
Korean hand needles, inserted into her at a 70-80 degree angle about
1-3mm. The pre-operative acupuncture treatment was for 1 hour. A pre-anesthetic
injection of hydromorphone and midazolam was given 30 minutes prior
to surgery. The hydromorphone was diluted to 0.05mg/ml and the dose
was 0.1mg/kg. The midazolam was diluted to 0.05mg/ml and given at a
dose of 0.1mg/kg.
Preoperative
care consisted of a 90F water soaking and dry-needling acupuncture,
approximating bilateral points BL21 and BL25. Needles used were 0.18mm
Korean hand needles, inserted into her at a 70-80 degree angle about
1-3mm. The pre-operative acupuncture treatment was for 1 hour. A pre-anesthetic
injection of hydromorphone and midazolam was given 30 minutes prior
to surgery. The hydromorphone was diluted to 0.05mg/ml and the dose
was 0.1mg/kg. The midazolam was diluted to 0.05mg/ml and given at a
dose of 0.1mg/kg. 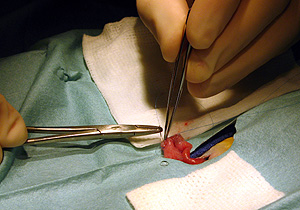 A
2-3cm paramedian incision was made 3-4mm from the caudal abdominal vein
and the celom was entered. The bowel was very large but was gently pulled
out of the celom and rotated to get maximal exposure. The exposed bowel
was very firm and had no obvious vessels over the sand impacted areas.
Since the entire length was filled with sand it was difficult to incise
aboral to the impaction. An enterotomy was performed, incising just
aboral to the impaction and then going orally about 1.5 cm into the
impacted area (about the same length as the width of the impaction.
Five large chunks of walled off sand were gently removed from the bowel.
A
2-3cm paramedian incision was made 3-4mm from the caudal abdominal vein
and the celom was entered. The bowel was very large but was gently pulled
out of the celom and rotated to get maximal exposure. The exposed bowel
was very firm and had no obvious vessels over the sand impacted areas.
Since the entire length was filled with sand it was difficult to incise
aboral to the impaction. An enterotomy was performed, incising just
aboral to the impaction and then going orally about 1.5 cm into the
impacted area (about the same length as the width of the impaction.
Five large chunks of walled off sand were gently removed from the bowel.
 The
enterotomy was closed using 7-0 prolene in a simple continuous pattern
and followed by a chushings inverting oversew.
The
enterotomy was closed using 7-0 prolene in a simple continuous pattern
and followed by a chushings inverting oversew. 
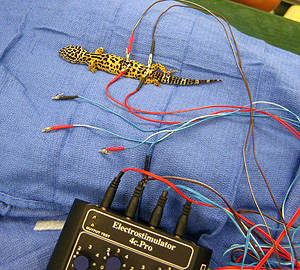 Post
operatively, Rocky was kept on oxygen while we placed again 0.18mm acupuncture
needles at approximately bilateral points BL21 and BL25. Electrical
stimulation of these points BL21->BL25 was performed to help relieve
the foreseeable ensuing illeus.
Post
operatively, Rocky was kept on oxygen while we placed again 0.18mm acupuncture
needles at approximately bilateral points BL21 and BL25. Electrical
stimulation of these points BL21->BL25 was performed to help relieve
the foreseeable ensuing illeus.  A
Patheon electric stimulater was used and points stimulated at 4-10Hz
for fifteen minutes during recovery. Once Rocky was alert and responsive
the needles were removed and a post operative temperature was taken
(infrared) and temp was 89F. Rocky's post operative weight was 19g which
means she had eaten more than half her body weight in sand!
A
Patheon electric stimulater was used and points stimulated at 4-10Hz
for fifteen minutes during recovery. Once Rocky was alert and responsive
the needles were removed and a post operative temperature was taken
(infrared) and temp was 89F. Rocky's post operative weight was 19g which
means she had eaten more than half her body weight in sand!